
193 results
Inequality on the frontline: A multi-country study on gender differences in mental health among healthcare workers during the COVID-19 pandemic
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 11 / 2024
- Published online by Cambridge University Press:
- 04 March 2024, e34
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Expectations and perspectives of cognitive behavioural therapy for childhood anxiety and related disorders
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 52 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 13 September 2023, pp. 65-77
- Print publication:
- January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
“Asking for help, quite a challenge”. Time from onset of symptoms to consultation with a psychiatrist
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S469-S470
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
One of the biggest challenges for primary care professionals is to know when it is appropriate to request a consultation with a psychiatrist. A complete medical history should be performed to detect anxious-depressive symptoms, as well as to determine the intensity, the trigger, time of evolution, and the functional repercussion (1). It is also important that the patient is able to express his or her symptoms and ask for help. The concept of “Alexitimia” refers to the difficulty of expressing feelings verbally, and is a frequent symptom in depressive patients (2).
In mild cases and with little repercussion, the physician himself can initiate treatment and follow up (3). However, on other occasions, it will be advisable to request a consultation with psychiatry.
ObjectivesThe main objective is to observe the time that elapses from the onset of symptoms until consultation with the Mental Health team is finally requested. Some preliminary results can already be obtained from this data collection.
MethodsWe have decided to carry out a descriptive study, collecting different variables from patients attending a first Psychiatry consultation.
ResultsIn a total sample of 208 patients, the majority (67%) were between 31 and 60 years old. Following the DSM-V criteria (4), patients were classified into groups according to their disorder: Adaptive, depressive, or other. These data were cross-referenced (Figure 1).
Subsequently, the time elapsed from the onset of symptoms (referred by the patients) was collected, until the referral to Psychiatry was processed. In order to make a comparison, average time (in days) was calculated for the different groups according to their age and diagnosis.
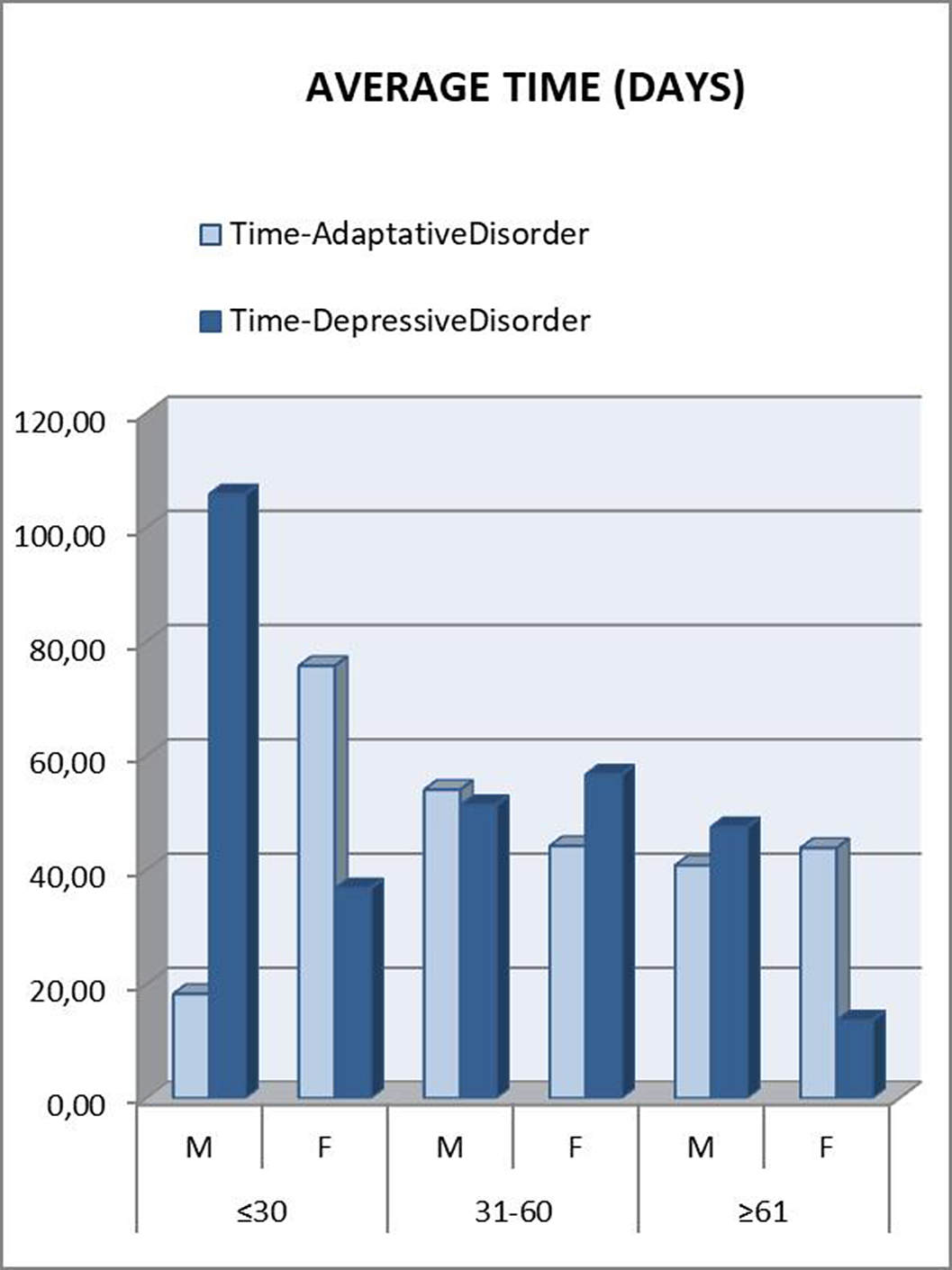
Those patients under 30 years were referred to psychiatry later. A downward trend was seen as the age range increased. In the “younger than 30” and “between 31 and 60” groups, patients who met criteria for Depressive Disorder took longer to be referred, which was striking considering that they are usually considered as more severe patients (Figure 2). This can be attributed to a greater difficulty in expressing their emotions (alexithymia), as another depressive symptom. Disaggregating these data by gender, the patients who clearly took the longest to be referred were men under 30 years old with a final diagnosis of Depressive Disorder (Figure 3). This gender difference is consistent with the social impact of alexithymia according to some articles (5).
Image:
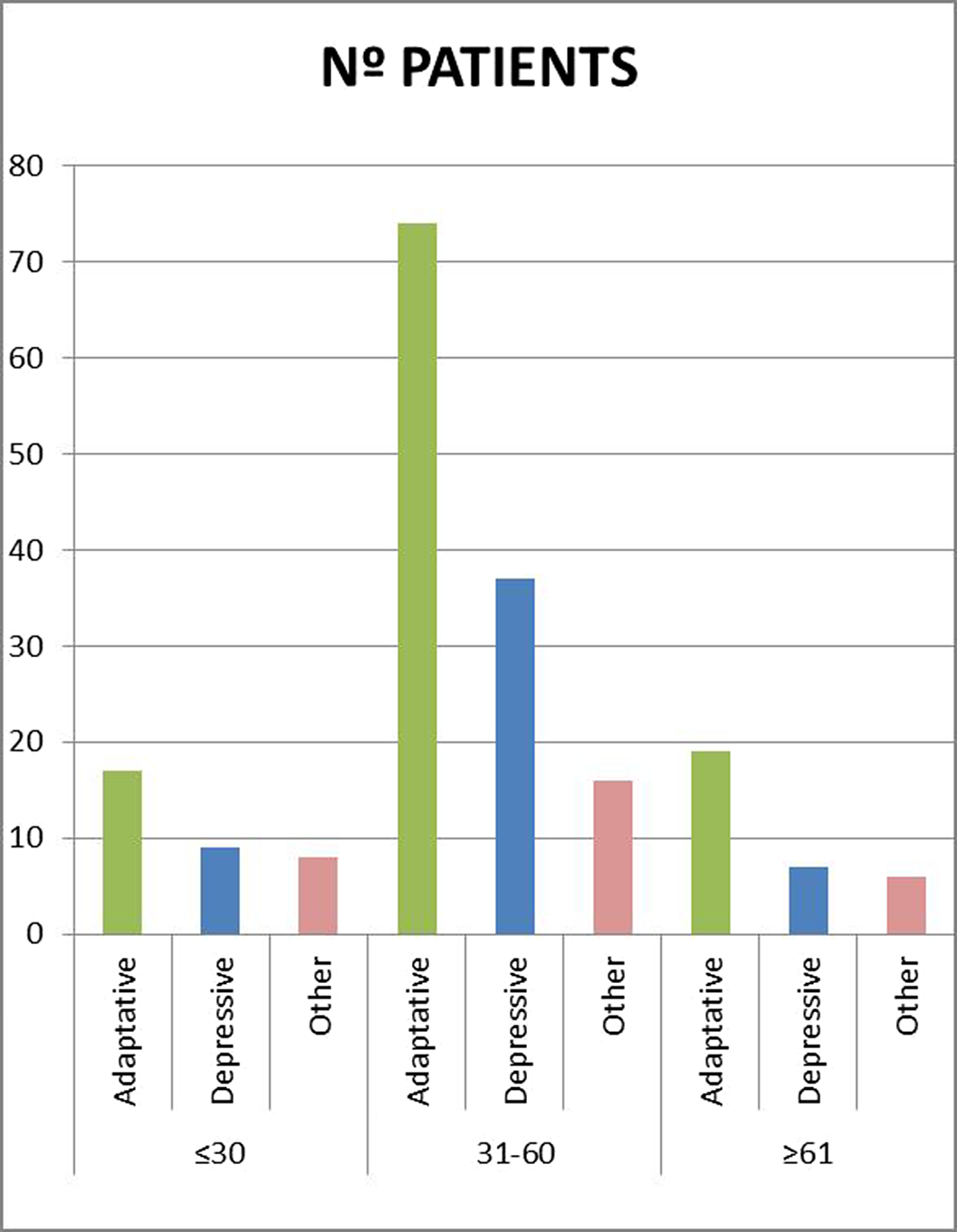
Image 2:
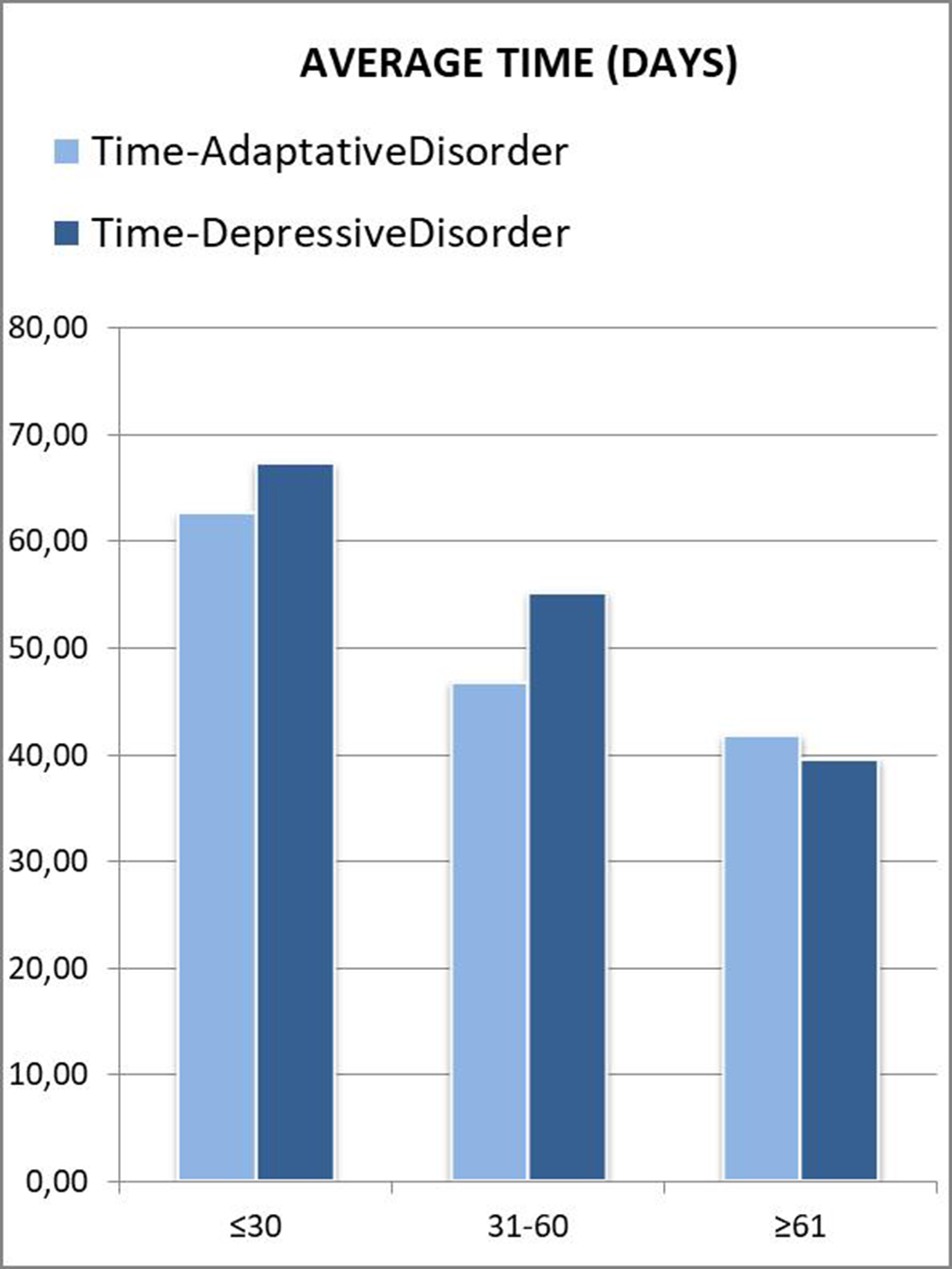
Image 3:
 Conclusions
ConclusionsIt is important that primary care physicians know how to take a complete history in those patients with symptoms of anxiety and depression.
In many cases, patients themselves have difficulties expressing their emotions and feelings (alexithymia), which may be another symptom of their discomfort.
This may lead to a delay in the time until referral to a psychiatry is requested, and therefore a worsening of symptoms.
Disclosure of InterestNone Declared



DOCTOR, I’M PREGNANT. Psychopharmacological treatment of depression in pregnant women. A clinical case of a pregnant woman and major depressive disorder
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1011
-
- Article
-
- You have access
- Open access
- Export citation
A cross-sectional descriptive study to assess the impact of the “open door” policy on patient satisfaction
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S910
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Since the beginning of the modern psychiatry the acute units have established a “locked door” policy. Some studies show that this condition may increase patient’s discomfort and affect the perception of health quality of care (Boyer L, 2009, Eur Psychiatry Dec;24(8):540-9). Lately, several European countries such as Germany, Switzerland and Spain are starting to implement the “open-door” policy but its impact on patient’s satisfaction is still unknown (Hochstrasser, L, Frontiers in Psychiatry, 9(57). https://doi.org/10.3389/fpsyt.2018.00057) .
ObjectivesTo help characterize the advantages of the “open-door” policy implemented in an acute inpatient psychiatric unit in order to assess the patient’s view of it.
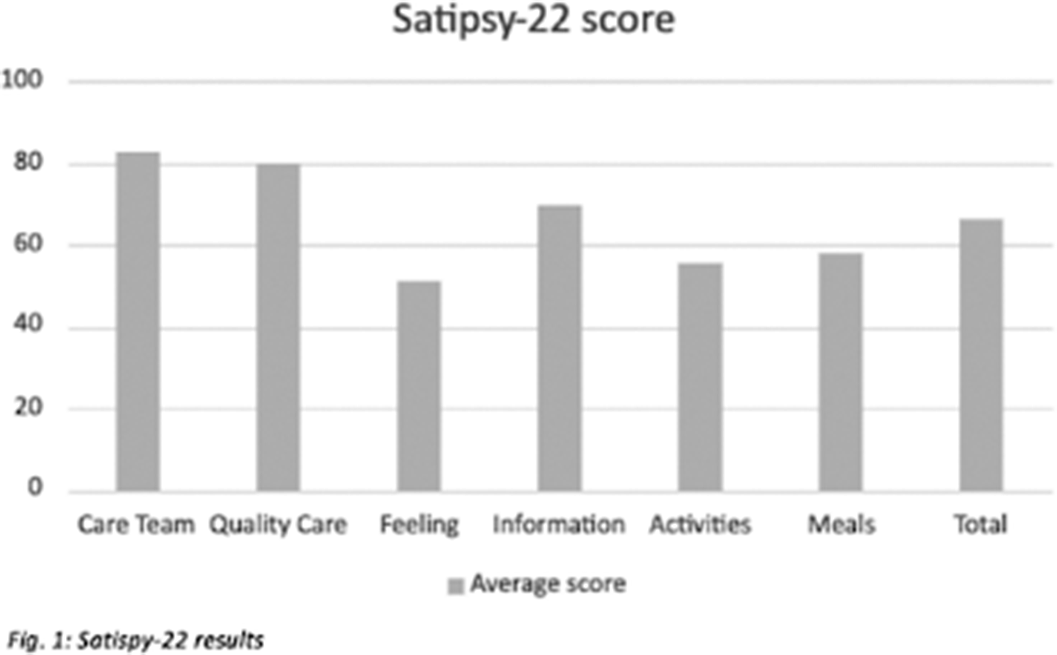
MethodsThis is a descriptive observational study carried out at an inpatient psychiatric unit. Data were collected after the implementation of the open door policy on June 2019, assessing the patient satisfaction of 31 subjects who completed the SATISPSY-22 scale at the time of discharge. Results are described using the average and its standard deviation.
ResultsResults show scores in all items above 50 points, being the care team and the quality of care the most valued ones with 82 and 79 points respectively. The overall score is above 65 points (Fig. 1).
Image:
 Conclusions
ConclusionsIn line with previous studies, our data suggests that the main impact of the “open-door” policy implementation is on patients’ perception of the care, being Quality of care and satisfaction with the Staff the items with highest scores. This could be explained by patients trusting more in the Care team, which would help enhance the therapeutic relationship improving therapeutic adherence, treatment adequacy and the outcome. Nevertheless, the Feeling related to hospitalisation was found to be the item with the lowest score. This could mean strategies should focus on improving patient’s insight regarding their clinical state and their need to be admitted. Our study supports the hypothesis that open-door policy in acute psychiatric units is seen positively by patients and that further research should be carried.
Disclosure of InterestNone Declared

A tale of excess: the curious case of the woman with 1447 emergency visits
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S286
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Frequent attenders to emergency services are challenging and costly. We report the case of a woman in her mid-twenties who stands out for a total of 1447 emergency visits.
ObjectivesOur primary objective was to describe the emergency visits of our patient. Secondary objectives were to assess her use of other healthcare services and to calculate her health expenditure.
MethodsThis is a clinical case report. We reviewed the patient’s electronic medical records for sociodemographic and clinical data. We obtained detailed information of psychiatric ED visits (length, most frequent times and days) regarding the second most-visited hospital. We assessed the efficacy of hospitalizations in reducing ED visits with a paired samples t Test, comparing the number of visits 30 days pre- and post-hospitalization. We estimated the health expenditure using the regional public health system prices, including three direct costs: emergency visits, hospitalizations and ambulance transportation. We obtained written informed consent from the patient’s legal guardian.
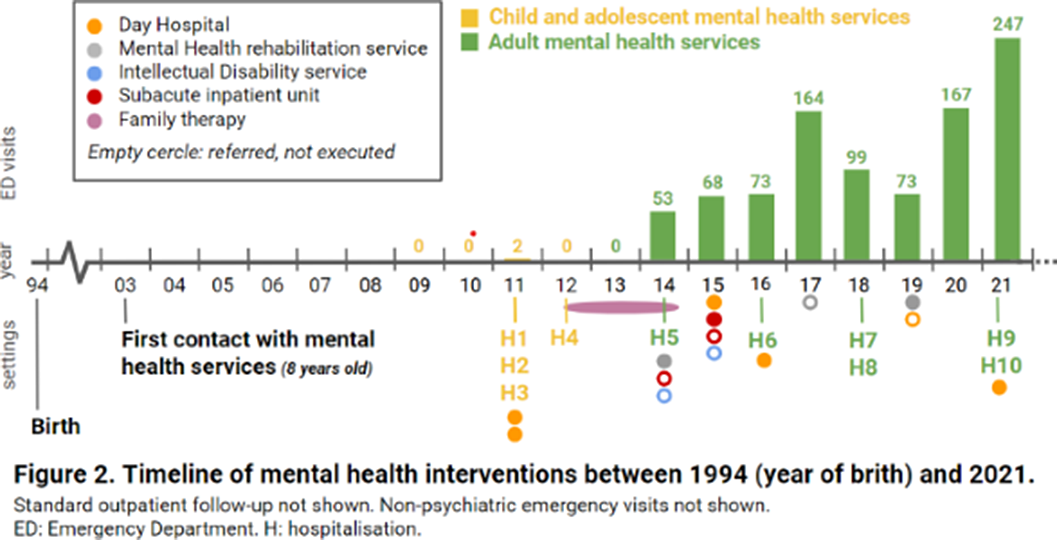
ResultsA 26-year-old woman from Barcelona (Catalonia, Spain), diagnosed with mild intellectual disability, made 1447 emergency visits between 2009 and 2021 (figure 1). 946 visits (65%) took place in psychiatric emergency departments (EDs), whilst 353 (24%) in non-psychiatric EDs and 148 (10%) in urgent primary care. She attended 24 hospitals (ranking number one the closest to the patient’s home, with 387 visits) and seven primary care centers, distributed across 17 cities in Catalonia. Most visits were self-referred, being the main presenting problems anxiety and instrumental suicidal behaviour. Saturday was her favorite day for hospital visits (24,1%), while she seeked care on Tuesdays much less often (4.5%). She made 73.5% of consultations between 1pm and 6pm, with a median length per visit of 2.8 hours (range 0.33-20.9 hours). Regarding other therapeutic approaches, she attended day hospitals, psychiatric rehabilitation programs and family therapy, among others (figure 2), for which she showed low adherence and scarce benefit. She had ten acute hospitalizations, interventions that did not reduce ED visits (t=-0.9835, p=0.36). Health expenditure reached 410.035€.
Image:
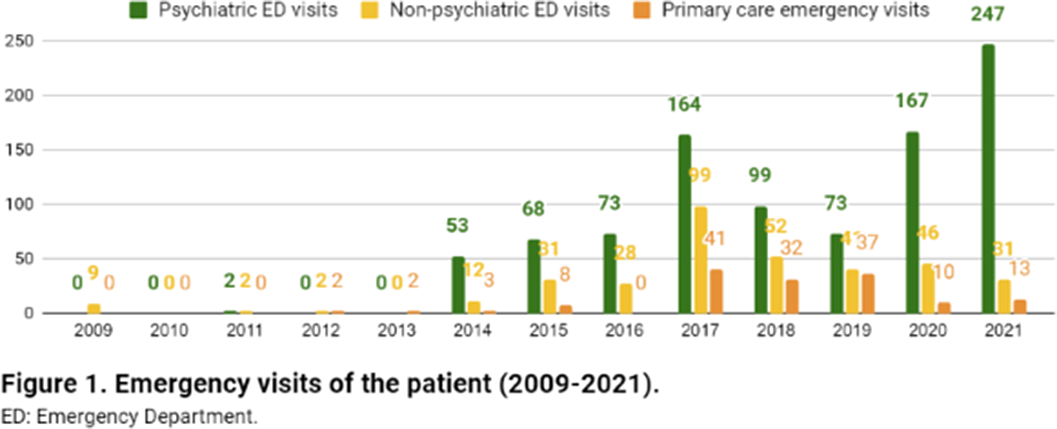
Image 2:
 Conclusions
ConclusionsThe most common definition of frequent attendance is a patient who has five or more visits per year. Many times, but not always, repeat visits are also inappropriate. The case we report is a grotesque example of both frequent and inappropriate attendance, which has been resistant to all kinds of interventions and has quality-of-care, financial and ethical implications. As of today, it is still a pending case. Maybe it is worth considering residential treatment?
Disclosure of InterestNone Declared


Efficacy of maintenance electroconvulsive therapy in recurrent depression: a case series
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S832
-
- Article
-
- You have access
- Open access
- Export citation
UNTIL IT BURSTS OR ALL OF US BURST. A SCHIZOTYPICAL CASE.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S967
-
- Article
-
- You have access
- Open access
- Export citation
The silent waitress. A case report of mutism without catatonia
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S627-S628
-
- Article
-
- You have access
- Open access
- Export citation
Delirious episode secondary to rotigotine: the psychotic patch
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S626
-
- Article
-
- You have access
- Open access
- Export citation
Bipolar disorder and substance use: Risk factors and prognosis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S704
-
- Article
-
- You have access
- Open access
- Export citation
Correlation between BDNF levels and folic acid levels at baseline in drug-naïve First Episode Psychosis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S184-S185
-
- Article
-
- You have access
- Open access
- Export citation
I don’t know where I’m going or where I come from. Self-disorders in schizophrenia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1069-S1070
-
- Article
-
- You have access
- Open access
- Export citation
Conversive and Factitious disorders: Differential diagnosis based on a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S687
-
- Article
-
- You have access
- Open access
- Export citation
PEAKS AND VALLEYS: BIPOLAR DISORDER, RAPID CYCLERS AND ENERGY DRINKS CONSUMPTION
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S702-S703
-
- Article
-
- You have access
- Open access
- Export citation
Late diagnosis of attention deficit hyperactivity disorder and cocaine abuse
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S335-S336
-
- Article
-
- You have access
- Open access
- Export citation
Memory complaints and quality of life in a patient with mild cognitive impairment
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S937-S938
-
- Article
-
- You have access
- Open access
- Export citation
“The cat and the calcium”. A case of delirium secondary to hypercalcaemia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S946-S947
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Interconsultation with the psychiatry service is frequently requested from other specialties for the assessment and treatment of patients who present neuropsychiatric symptoms secondary to organic alterations. On the other hand (and in relation to this case), within the possible causes for the elevation of calcaemia figures, the most frequent are hyperparathyroidism and neoplasms, representing between these two entities 90% of cases (1).
Among the organic mental disorders, Delirium stands out, with an approximate prevalence between 1 and 2% (general population), which increases in hospitalized and elderly patients (2).
ObjectivesPresentation of a clinical case about a patient with delirium secondary to hypercalcemia, with hallucinations and behavioral disturbance.
MethodsBibliographic review including the latest articles in Pubmed about delirium (causes and treatment) and hypercalcaemia secondary to neoplasms.
ResultsWe present a 52-year-old male patient, who went to the emergency room accompanied by his wife, due to behavioral alteration. Two days before, he had been evaluated by Neurology, after a first epileptic crisis (with no previous history) that resolved spontaneously. At that time, it was decided not to start antiepileptic treatment.
The patient reported that he had left his house at midnight, looking for a cat. As he explained, this cat had appeared in his house and had left his entire bed full of insects. His wife denied that this had really happened, and when she told the patient to go to the emergency room, he had become very upset.
As background, the patient used to consume alcohol regularly, so the first hypothesis was that this was a withdrawal syndrome. However, although the consumption was daily, in recent months it was not very high, and at that time no other symptoms compatible with alcohol withdrawal were observed (tremor, tachycardia, sweating, hypertension…).
We requested a general blood test and a brain scan. The only relevant finding was hypercalcaemia 12.9mg/dL (which could also be the origin of the previous seizure). It was decided to start treatment with Diazepam and Tiapride in the emergency room, with serum perfusion, and keep under observation. After several hours, the patient felt better, the hallucinations disappeared, and calcium had dropped to 10.2mg/dL. A preferential consultation was scheduled, due to suspicion that the hypercalcaemia could be secondary to a tumor process.
Image:
 Conclusions
ConclusionsIt is important to rule out an organic alteration in those patients who present acute psychiatric symptoms. Hypercalcaemia is frequently associated with tumor processes (1) due to secretion of PTH-like peptide (4), so a complete study should be carried out in these cases.
Delirium has a prevalence between 1 and 2% in the general population (2).
Psychopharmacological treatment is used symptomatically, with antipsychotics (3). For the episode to fully resolve, the underlying cause must be treated.
Disclosure of InterestNone Declared

Double dystonia secondary to risperidone: acute laryngeal dystonia and oculogyric crisis.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1066
-
- Article
-
- You have access
- Open access
- Export citation
“Keeping an eye on amylase”. Side effects of antidepressants
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S831
-
- Article
-
- You have access
- Open access
- Export citation
